Handbook of Structural Brain MRI Analysis
by Jerome J Maller BScGradDipPsychMScPhD
with contributions by Rodney Anderson BSc(HonsPsych), Melissa Kirkovski PhD, Phillip Law PsycSc(Hons), Kerstin Pannek PhD, Caley Sullivan BA/BSc(Hons), Jonatan Ottino-Gonzalez MSc, and Thomas Welton BScMScPhD.
Here is Part I

|
Jeromes_Structural_MRI_analysis_handbook_October2019_Part1.pdf Size : 3647.085 Kb Type : pdf |
Here is Part II (Tractography)
|
|
Jeromes_Structural_MRI_analysis_handbook_April2017_Part2.pdf Size : 2889.529 Kb Type : pdf |
Here is part 3: How to make a Linux Virtual Machine for MRI data analysis
|
|
Jeromes_Structural_MRI_analysis_handbook_October2019_Part3.pdf Size : 264.186 Kb Type : pdf |
Acknowledgements
We would like to acknowledge Chantal Réglade-Meslin, Paul Fitzgerald, Stephen Rose, Joshi George Cherayath, Kaarin Anstey, Wei Wen, Jiyang Jiang, Richard Nibbs and Carsten Liess for their technical assistance and ongoing support. We would also like to thank the many people whose MRI brain scans we have acquired and analyzed.
List of abbreviations
ASL=Arterial spin labelling; CSF=Cerebrospinal fluid; DICOM= Digital imaging and communications in medicine; DTI=Diffusion tensor imaging; DWI=Diffusion weighted imaging; FLAIR=Fluid attenuated inversion recovery; GM=Grey matter; GUI=Graphical user interface; ICV=Intracranial volume; MPRAGE=Magnetization prepared rapid acquisition gradient recall echo; MP2RAGE=MPRAGE with multiple inversion times; MRI=Magnetic resonance imaging; Nifti= Neuroimaging informatics technology initiative; ROI=Region of interest; SPGR=Spoiled gradient; SWI=Susceptibility weighted imaging; TBV=Total brain volume; VM=Virtual machine; WM=White matter
Preface
Have you ever spent hours going through long software manuals and endless forums trying to work out how to analyze structural MRI scans? We used to do that too, so over time we have documented how to use a wide variety of software packages so we could conduct the analyses we wanted to carry out. We have also received training in some of these packages which has enhanced our competence in these programs.
We don't claim to know how to use every module of every program, but we know how to use them to conduct most of the analyses that you are likely to want to run. We have utilized what we’ve learnt by publishing dozens of peer-reviewed papers but also passing on this skill set to many students and research groups around the world.
Chapter 1 of this Handbook focuses on step-by-step instructions on how to use various packages to process structural MRI data.
Chapter 2 of this Handbook focuses on white matter anatomy and the placement of region-of-interest seeds using diffusion MRI data to perform tractography.
Chapter 3 of this Handbook describes how to setup a virtual machine with software necessary to process structural MRI data.
CHAPTER 1
Introduction
Whilst there are many packages available, we have found that those we describe in this handbook have collectively been sufficient to analyze structural MRI scans. However, we encourage you to seek alternative packages if you do not find these ones adequate to accomplish your tasks.
In this handbook, we provide step-by-step instructions for how to use your data to achieve the output you require. The focus of this handbook is T1-weighted and Diffusion data acquisition and analysis.
Topics covered in this handbook
- Minimum computer specifications
- Installation of these packages
- T1-weighted and Diffusion Tensor Imaging
- Other structural sequences to consider
- What is T1-weighted useful for?
- What is DTI useful for?
- Issues to consider before acquisition
- Software
- Pipelines/scripts to save you time
Minimum computer specifications
Windows (pc), Linux/Unix, Macintosh/Apple
The bare minimum specifications are Core2Duo CPU with 4GB RAM, but, of course, it’s best to have the fastest and most amount of RAM you can access. Same goes for the hard drive capacity: at least 250GB but the bigger the better!
Although you could have a pc running Windows and Linux through a virtual machine (VM), this is not an ideal setup as VMs are notoriously slow. By contrast, a dual-booting pc would be far preferable (this is, Windows and Linux on the same pc with a simple boot menu when you turn on the pc). If you have a Mac/Apple, then the best setup is to run the Mac OS natively and then install dual-boot software such as Bootcamp or Parallels and then install Windows onto that. Note the Mac/Apple is essentially running on Linux, so you simply open a terminal and you immediately have Linux running natively – very handy. Windows 10 offers a Linux kernel.
Of course, if you have access to a supercomputer/cluster via the university then you could run all of your analyses on it, but note that those huge mainframes sometimes have problems and need to shut down to reboot which will interfere with your batched analyses.
Note that not all MRI analysis packages are multi-threaded i.e. they do not use more than one CPU core at a time, whereas those that are multithreaded can utilise as many CPUs (and cores) as you have available on the computer. Again, very handy.
Installation of these packages
Most of these packages are simple executable (.exe) files than run natively on Windows. However, some run only on Linux/Mac (e.g. FSL, FreeSurfer) so need to be installed/compiled with the correct paths and calling the correct files; sometimes you will need to install updates via apt-get. Some (e.g. FreeSurfer) run in separate shells (e.g. tcsh or csh). If you are a Linux/Mac user, you may find it convenient to run the Windows packages via VMs, or use windows emulators such as wine.
T1-weighted and Diffusion Tensor Imaging (DTI)
Without going into the physics of it, T1-weighted is essentially the sort of scan you acquire if you want data with good grey/white matter contrast. The word ‘contrast’ is this context means the clarity of the grey/white matter (and CSF) borders. This is very important when segmenting regions of interest (ROIs) as they rely on clear grey/white matter borders. However, the clarity of these borders is also important in the clinical context as a lack of contrast between grey/white matter can sometimes indicate poor structural integrity as sometimes seen, for example, after traumatic brain injury (TBI). A type of MRI sequence that investigates this more thoroughly is referred to as MTR (magnetisation transfer ratio), but that’s beyond the scope of this handbook.
Diffusion tensor imaging (DTI) was released in 1994 by Basser and colleagues but not utilised widely until processing power dramatically increased in the early 2000’s (see our article reviewing this, Maller et al., 2010). Filler (2009) provides a comprehensive description of its origins. It is based upon DWI (diffusion weighted imaging) but instead of 2-dimensional data, DTI acquires 3-dimensional data (or 4-dimensional, depending on how you look at it). Essentially, DTI produces data that is based upon Brownian movement i.e. the movement of water between microscopic white matter fibres based on heat. Water will move in a straight line that is directly parallel to the direction of the white matter when the white matter is ‘healthy’, but the water will move in different directions when the white matter’s "integrity" is compromised. As an analogy, think of a bowl of spaghetti… Another useful analogy is a hose with water flowing through it: when the hose is new and has no leaks the water will move parallel to the hose, that is, in an anisotropic direction. Isotropic means the water is moving equally in all directions, hence, anisotropic means in one single direction. When a white matter bundle is damaged, it may be compressed or stretched, leading to leaking in that white matter bundle – this will cause the water flowing within it to leak out the side or its flow obstructed, leading to the water flow not being parallel anymore to the shape of the hose i.e. the white matter bundle. When the water flows parallel to the hose in one direction, the ‘fractional anisotropy’ (FA) has a value close to 1; when the hose is leaking and the water flows in all directions equally (e.g. up, down, out the sides), the FA is closer to 0.
The basic physics of NMR is nicely demonstrated here: http://www.youtube.com/watch?v=1OrPCNVSA4o
Other structural sequences to consider
- T2-weighted, T2-FLAIR, susceptibility-weighted imaging (SWI), arterial spin labelling (ASL)
- T2-weighted is a scan acquired when you want to look at possible pathology, for example, white matter hyperintensities (WMHs), strokes, tumours, cysts, etc. In normal ageing, WMHs first appear lining the inner border of the lateral ventricles, referred to as periventricular leukomalacia (PVL), which often begins after the age of 40. Large WMHs within cortical or subcortical matter are often representative of pathology, although WMH ‘dots’ can be as well (sometimes referred to as ‘punctate’). For example, these can be representative of white matter disease sometimes related to late-onset major depression. The rule-of-thumb is that one WMH per decade is within acceptable limits. T2-FLAIR is like a T2-weighted scan but the colour of the cerebrospinal fluid (CSF) is inverted. That is, instead of CSF appearing white, it is black on a FLAIR scan. Hence, FLAIR stands for FLuid Attenuated Inversion Recovery. SWI focuses on the susceptibility of iron and myelination, hence, it is “susceptible” to alterations in iron and myelination. ASL is a sequence used to assess absolute measures of blood flow, rather than relative blood flow such as in dynamic contrast enhanced MRI (DCE-MRI). However, ASL is associated with quite high SAR (specific absorption rate), so sequences cannot be too long, hence variations (such as pseudo continuous ASL, pCASL) is often preferred.
What is T1-weighted useful for?
- T1-weighted data has a variety of uses, but in the research context, it is used mostly for investigating grey matter (GM), white matter (WM), CSF, and atrophy.
- Volumetrics; GM+WM+CSF=intracranial volume (ICV). Total brain volume (TBV)/ICV = opposite of CSF/ICV. That is, TBV/ICV is a measure of how much of the cranial vault contains brain matter, whereas the opposite (CSF/ICV) is a measure of how much of the cranial vault is not brain matter; hence, CSF/ICV is sometimes referred to as a measure of atrophy. Note that some programs (e.g. FreeSurfer) yield data of TBV and ICV but the TBV does not include blood vessels, choroid plexus, non-brain matter constituents, hence, TBV/ICV in those programs will be smaller than programs that assume everything within the cranial vault is either brain matter or CSF (e.g. FSL’s FAST module, or SPM’s segment routine).
- Thickness. Cortical thickness is representative of how thick the cortical grey matter is. Essentially, volume = thickness x area.
- Curvature/shape analysis can also be accomplished with T1-weighted data, but its meaning is less straight forward.
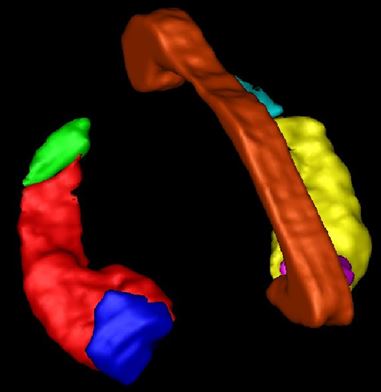
What is DTI useful for?
- WM Structural integrity and directionality
- FA, L1 (λ1), L2 (λ2), L3 (λ3), MD, RD. Figure 1 illustrates what the eigenvalues (λ) represent (from Maller et al.,2010).
- Tractography of WM bundles
- Connectivity
- Fibre density
Issues to consider before acquisition
- Scanner type (brand, Tesla, gradients, acquisition pulse sequences installed onto the console)
- SPGR (spoiled gradient, used with GE scanners), MPRAGE (Magnetization Prepared Rapid Acquisition GRE (3D Inversion Recovery)), MP2RAGE (MPRAGE with multiple echoes; MPRAGE and MP2RAGE are used with Siemens and Philips scanners but recently also on GE scanners)
- DTI, RESOLVE (used for high-resolution q-ball scanning that takes into account crossing fibres)
- Silenz (GE) and PETRA (Siemens) – these are T1-weighted sequences that are less than 10db above ambient noise level
- Fast scanning/GRAPPA, SENSE, SMASH, PILS etc. These usually are parallel imaging methods to reduce scanning times although they can also reduce SNR. MRI is always about give-and-take in terms of SNR
- Fat suppression and chemical shift
- NEX/number of averages – the more averages, the higher the SNR
- Number of channels (receive coils i.e. antennae) – the more channels the better the resolution but also sometimes lower SNR
- Resolution, repetition time (TR), echo time (TE), slice thickness, signal-to-noise ratio (SNR) – TE can be altered, for example, but must not change between subjects, slice thickness should be less than 1.5mm for T1-weighted and no more than 3mm for DTI
- DTI number of directions: more directions will yield more accurate tractography (but not necessarily more accurate FA estimation), and more b-zero volumes (T2-weighted scans) will yield better eddy current and movement correction especially when they are interleaved
- Anterior commissure-posterior commissure (AC-PC) alignment – important because if you normalize scans to a template then this will make the analyses more accurate with higher SNR as the scans will not have to be reorientated to match the template. AC-PC alignment in the scanner is also important because then you can more accurately compare data across scans
- Length of scanning period and each sequence – some people will not be able to remain very still for long periods of time, plus longer scans distribute more SAR
- Volume of scanner/patient comfort/movement – wide bore scanners are preferable for patient comfort and the ability to put more equipment into the scanner; patient movement will reduce the quality of the scans
- Knowing for sure which is right and which is left – sometimes software can flip the MRI scan, so it is useful to use fiducials (markers) that show on the scan so that you can always be sure which side is left and which side is right. For example, you can tape a vitamin E pill to the forehead above the right of the subject’s eyebrow before they are scanned so that the right-side of the scan (head) can always been confirmed.
Software covered in this handbook
- MRIcro (visualization, preprocessing, manual segmentation, lesion overlay analysis; http://www.mccauslandcenter.sc.edu/mricro/ )
- MRIcron and dcm2nii (format conversion; http://www.mccauslandcenter.sc.edu/mricro/ )
- MRIreg (http://www.mccauslandcenter.sc.edu/mricro/ )
- BEAM (http://www.clinicalresearcher.org/software.htm )
- MRIconvert (slice conversion http://lcni.uoregon.edu/~jolinda/MRIConvert/ )
- ITK-SNAP (T1-weighted visualization http://www.itksnap.org/pmwiki/pmwiki.php )
- Not free: Analyze® (http://www.analyzedirect.com/ ). Analyze® is the gold standard in manual segmentation software. There is a large variety of freeware that can be used to accomplish a similar task, but Analyze® is established as the most comprehensive and user-friendly package for manual ROI segmentation. It has a number of modules other than the ROI module, but these are beyond the scope of this handbook.
- FreeSurfer (T1-weighted automated segmentation) and QDEC (FreeSurfer GUI for analysis http://freesurfer.net/ )
- SPIN (slice conversion and SWI editing http://www.mrimaging.com/category.103.html )
- DICOMsort (multi-platform, Linux, Mac, Windows, for sorting DICOM images by any of the values in the DICOM header. http://www.dicomsort.com )
- FSL (http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/ ): brain extraction tool (BET), fully automated segmentation tool (FAST), tract based spatial statistics (TBSS)
- DTIstudio (deterministic tractography https://www.dtistudio.org )
- MedINRIA (deterministic tractography http://www-sop.inria.fr/asclepios/software/MedINRIA/ )
- MRtrix (deterministic and probabilistic tractography http://www.mrtrix.org/ , http://www.brain.org.au/software/ )
- SPM (for normalization and GM/WM/CSF segmentation http://www.fil.ion.ucl.ac.uk/spm/ )
Pipelines/scripts will save you time
Once you learn how to use a program, particularly those installed in Linux/Unix/Mac, it will save you substantial time (and effort) by writing scripts to conduct multiple-step analyses for multiple scans. You just need to be confident in your scripting! An extreme example of this is referred to as a “pipeline”. A good example of utilising both T1-weighted data and DTI data in one ‘program’ is referred to as the “Connectome pipeline” and another is TRACULA (TRActs Constrained by UnderLying Anatomy; http://surfer.nmr.mgh.harvard.edu/fswiki/Tracula ), although they may rely on you first processing the T1-weighted data through Freesurfer and then inputting the output of that process along with the DTI dataset into the pipeline.
WM bundles: getting to know white matter anatomy
A widely used reference for this is the White Matter Atlas by Mori et al. (2005), but there are many other white matter atlases/articles well worth considering as well, including, Wycoco et al. (2013). We encourage you to search on PubMed using keywords such as “white matter atlas” (http://www.ncbi.nlm.nih.gov/pubmed/?term=white+matter+atlas ). At the end of this handbook we have included some general advice on where to place initial seed points for a variety of major WM bundles.
Index of software
- How to convert individual dicoms (slices) into an analyze volume (.hdr + .img): MRIcro
- Steps to convert dicoms to Analyze format (.img + .hdr) with dcm2nii
- Preparing a T1-weighted scan for MiniBIRD
- Using the Ascension® MiniBIRD (Flock of Birds) for stereotaxic coregistration of MRI-to-head-and-brain
- How to locate the DLPFC (F3 or F4) without an MRI brain scan
- MRIconvert
- Example of tracing an ROI in MRIcro. In this case, the caudate.
- Manual tracing of a Region Of Interest (ROI) in Analyze®
- Steps for 3D rendering in ITK-SNAP of ROI (object maps) traced in Analyze
- Inter-rater reliability
- FreeSurfer
- Protocol to process SWI images from magnitude and phase data
- SPIN to convert a directory of DICOMS containing different sequences (series)
- DICOMsort (a multi-platform alternative to SPIN) to convert a directory of DICOMS containing different sequences (series) and anonymise data
- FSL
- Tract-Based Spatial Statistics (TBSS)
- DTIstudio: How to measure FA (and other statistics) of white matter tracts
- MedINRIA
- MRtrix
- Some useful Linux commands
- References
- Collection of our published articles that have used the software described in this handbook
- Imaging guide for tractography of major white matter fibre bundles
Collection of our published articles that have used the software described in this handbook
MRIcro and MRIreg
Fitzgerald PB, Fountain S, Hoy K, Maller JJ, Enticott P, Laycock R, Upton D, Daskalakis ZJ. (2007). A comparative study of the effects of repetitive paired transcranial magnetic stimulation on motor cortical excitability. Journal of Neuroscientific Methods 165(2): 265-9.
Fitzgerald PB, Daskalakis ZJ, Hoy K, Farzan F, Maller JJ. (2008). Cortical inhibition in motor and non-motor regions: a combined TMS-EEG study. Clinical EEG and Neuroscience 39(3):112-7.
Fitzgerald PB, Daskalakis ZJ, Hoy K, Farzan F, Maller JJ. (2009). GABA and cortical inhibition in motor and non-motor regions using combined TMS-EEG: A time analysis. Clinical Neurophysiology 120(9):1706-10.
Fitzgerald PB, Maller JJ, Hoy K, Thomson R, Daskalakis ZJ. (2009). Exploring the Optimal site for the Localization of Dorsolateral Prefrontal Cortex in Brain Stimulation Experiments. Brain Stimulation 2(4):237-9.
Fitzgerald PB, Hoy K, McQueen S, Maller JJ, Herring S, Segrave R, Bailey M, Been G, Kulkarni J, Daskalakis ZJ. (2009). A randomized trial of rTMS targeted with MRI based neuro-navigation in treatment-resistant depression. Neuropsychpharmacology 34(5):1255-62.
FreeSurfer
Buchanan B, Rossell S, Maller J, Toh W, Brennan S, Castle D. (2014). Regional brain volumes in body dysmorphic disorder compared to controls. Australian and New Zealand Journal of Psychiatry 48(7):654-62.
Calati R, Maller JJ, Meslin C, Lopez-Castroman J, Ritchie K, Courtet P, Artero S. Repatriation is associated with isthmus cingulate cortex reduction in community-dwelling elderly. The World Journal of Biological Psychiatry (In Press).
Grace SA, Buchanan B, Maller JJ, Toh WL, Castle DJ, Rossell SL. Reduced cortical thickness in body dysmorphic disorder. Psychiatry Research Neuroimaging 259:25-8.
Maller JJ, Anderson R, Thomson RH, Rosenfeld JV, Daskalakis ZJ, Fitzgerald PB. (2015). Occipital bending (Yakovlevian torque) in bipolar depression. Psychiatry Research: Neuroimaging 231(1):8-14.
Maller JJ, Anderson R, Thomson RHT, Daskalakis ZJ, Rosenfeld JV, Fitzgerald PB. Occipital bending in schizophrenia. ANZ Journal of Psychiatry (In Press).
Maller JJ, Thaveenthiran P, Thomson RH, McQueen S, Fitzgerald PB. (2014). Volumetric, cortical thickness and white matter integrity alterations in bipolar disorder Type I and II. Journal of Affective Disorders 168:118-27.
Maller JJ, Thomson RH, Pannek K, Bailey N, Lewis PM, Fitzgerald PB. (2014). Volumetrics relate to the development of depression after traumatic brain injury. Behavioural Brain Research 271:147-53.
Spitz G, Bigler ED, Abildskov T, Maller JJ, O’Sullivan R, Ponsford JL. (2013). Regional cortical volume and neuropsychological functioning following traumatic brain injury. Brain and Cognition 83(1):34-44.
Watson A, Croft R, Maller JJ, Fitzgerald PB. White matter correlates of episodic memory encoding and retrieval in schizophrenia. Psychiatry Research Neuroimaging 254:188-98.
FSL and/or DTIstudio and/or MRtrix
Buchanan BG, Rossell SL, Maller JJ, Toh WL, Brennan S, Castle DJ. (2013). Brain Connectivity in Body Dysmorphic Disorder Compared with Controls: A Diffusion Tensor Imaging Study. Psychological Medicine 43(12):2513-21.
Grieve SM, Maller JJ. High-resolution diffusion imaging – ready to become more than just a research tool in psychiatry? Molecular Psychiatry (In Press).
Kirkovski M, Enticott PE, Maller JJ, Rossell SL, Fitzgerald PB. (2015). Diffusion tensor imaging reveals no white matter impairments among adults with autism spectrum disorder. Psychiatry Research Neuroimaging 233(1):64-72.
Maller JJ. (2014). Neuroplasticity in normal and brain injured patients: Potential relevance of ear wiggling locus of control and cortical projections. Medical Hypotheses 83(6):838-43.
Maller JJ, Thaveenthiran P, Thomson RH, McQueen S, Fitzgerald PB. (2014). Volumetric, cortical thickness and white matter integrity alterations in bipolar disorder Type I and II. Journal of Affective Disorders 168:118-27.
Maller JJ, Thomson RHS, Pannek K, Rose SE, Bailey N, Lewis PM, Fitzgerald PB. (2014). The (eigen)value of diffusion tensor imaging to investigate depression after traumatic brain injury. Human Brain Mapping 35(1):227-37.
Spitz G, Maller JJ, O’Sullivan R, Ponsford JL. (2013). White matter integrity following traumatic brain injury: The association with severity of injury and cognitive functioning. Brain Topography. 26(4):648-60.
Analyze
Anstey KJ, Maller JJ, Réglade-Meslin C, Christensen C, Jorm AF, Wen W, Sachdev PS. (2004). Hippocampal and amygdalar volumes in relation to handedness in adults aged 60-64. NeuroReport 15(18):2825-29.
Anstey KJ, Mack HA, Christensen H, Li S, Reglade-Meslin C, Maller JJ, Kumar R, Dear KGB, Easteal S, Sachdev P. (2007). Corpus callosum size, reaction time speed and variability in mild cognitive disorders and in a normative sample. Neuropsychologia 45(8):1911-20.
Beauchamp MH, Anderson VA, Catroppa C, Maller JJ, Godfrey C, Morse S, Rosenfeld J, Haritou F, Kean M. (2009). Implications of reduced callosal area for social skills after severe traumatic brain injury in children. Journal of Neurotrauma 26(10):1645-54.
Beauchamp MH, Anderson VA, Catroppa C, Maller JJ, Godfrey C, Morse S, Rosenfeld J, Haritou F, Kean M. (2011). Structural brain changes persist 10 years after childhood traumatic brain injury. International Journal of Developmental Neuroscience 29(2):137-43.
Cyprien F, Courtet P, Malafosse A, Maller JJ, Meslin C, Bonafé, Le Bars E, Menjot de Champfleur N, Ritchie K, Artero S. (2011). Suicidal behavior is associated with reduced corpus callosum area. Biological Psychiatry 70(4):320-6.
Cyprien F, Courtet P, Poulain V, Maller JJ, Meslin C, Bonafé A, Lebars E, Ancelin M-L, Ritchie K, Artero S. (2014). Corpus Callosum size may predict late-life depression in women: a 10-year follow up study. Journal of Affective Disorders 165:16-23
Furtado C, Maller JJ, Fitzgerald PB. (2008). A MRI study of the Entorhinal Cortex in Treatment Resistant Depression. Psychiatry Research: Neuroimaging 163(2):133-42.
Furtado CF, Hoy KE, Maller JJ, Savage G, Daskalakis ZJ, Fitzgerald PB. (2011). Cognitive and volumetric predictors of response to repetitive transcranial magnetic stimulation (rTMS) – A prospective follow-up study. Psychiatry Research: Neuroimaging 202(1):12-19.
Furtado CP, Hoy KE, Maller JJ, Savage G, Daskalakis ZJ, Fitzgerald PB. (2012). An investigation of medial temporal lobe changes and cognition following antidepressant response: A prospective rTMS study. Brain Stimulation 6(3):346-54.
Green REA, Colella B, Maller JJ, Bayley M, Glazer J, Mikulis DR. (2014). Scale and pattern of atrophy in the chronic stages of moderate-severe TBI. Frontiers in Human Neuroscience 8(67):67.
Jorm AF, Butterworth P, Anstey KJ, Christensen H, Easteal S, Maller J, Mather KA, Turakulov RI, Wen W, Sachdev P. (2004). Memory complaints in a community sample aged 60-64 years: Associations with cognitive functioning, psychiatric symptoms, medical conditions, APOE genotype, hippocampus and amygdala volumes, and white-matter hyperintensities. Psychological Medicine 34(8):1495-1506.
Looi JCL, Lindberg O, Liberg B, Tatham V, Kumar R, Maller JJ, Millard E, Sachdev P, Hogberg G, Pagani M, Botes L, Engman E-L, Zhang Y, Svensson L, Wahlund L-O. (2008). Volumetrics of the caudate nucleus: reliability and validity of a new manual tracing protocol. Psychiatry Research Neuroimaging 163(3):279-288.
Looi JCL, Tatham V, Kumar R, Maller JJ, Millard E, Wen W, Brodaty H, Sachdev P. (2009). Caudate nucleus volumes in stroke and vascular dementia. Psychiatry Research Neuroimaging 174(1):67-75.
Looi JC, Maller JJ, Pagani M, Högberg G, Lindberg O, Liberg B, Botes L, Engman EL, Zhang Y, Svensson L, Wahlund LO. (2009). Caudate volumes in public transportation workers exposed to trauma in the Stockholm train system. Psychiatry Research 171(2):138-43.
Maller JJ, Réglade-Meslin C, Anstey KJ, Sachdev PS. (2006). Sex and symmetry differences in hippocampal volumetrics: Before and beyond the opening of the crus of the fornix. Hippocampus 16(1):80-90.
Maller JJ, Meslin C, Anstey KJ, Wen W, Sachdev PS. (2007). Hippocampus and amygdala volumes in a random community-based sample of 60-64 year olds and their relationship to cognition. Psychiatry Research Neuroimaging 156(3):185-97.
Maller JJ, Daskalaskis ZJ, Fitzgerald PB. (2007). Hippocampal volumetrics in depression: the importance of the posterior tail. Hippocampus 17(11):1023-7.
Maller JJ, Réglade-Meslin C, Chan P, Daskalakis ZJ, Thomson RH, Anstey KJ, Budge M, Sachdev P, Fitzgerald PB. (2011). Hippocampal sulcal cavities: prevalence, risk factors and relationship to memory impairment. Brain Research 1368:222-30.
Maller JJ, Daskalakis ZJ, Thomson RHS, Daigle M, Barr MS, Fitzgerald PB. (2012). Hippocampal volumetrics in treatment-resistant depression and schizophrenia: The Devil’s in de-tail. Hippocampus 22(1):9-16.
Maller JJ, Reglade-Meslin C, Thomson RHS, Daigle M, Barr MS, Daskalakis ZJ, Fitzgerald PB. (2013). Hippocampal sulcal cavities in depression and healthy individuals. Journal of Affective Disorders 150(3):785-9.
Maller JJ, Reglade-Meslin, C. (2014). Longitudinal hippocampal and fornix changes after traumatic brain injury: Observations from traditional structural magnetic resonance imaging. Journal of Neurology and Neurophysiology 5(1):1-8.
Maller JJ, Thomson RHS, Rosenfeld JV, Anderson R, Daskalakis ZJ, Fitzgerald PB (2014). Occipital bending in depression. Brain 137(Pt 6):1830-7.
Maller JJ, Anderson R, Thomson RHS, Daskalakis ZJ, Rosenfeld JV, Fitzgerald PB. Occipital bending in schizophrenia. ANZ Journal of Psychiatry (In Press).
Miller LS, Collela B, Mikulis D, Maller J, Green REA. (2013). Environmental enrichment may protect against hippocampal atrophy in the chronic stages of traumatic brain injury. Frontiers in Human Neuroscience 7(1):1-8.
Ritchie K, Jaussent I, Portet F, Courtet P, Malafosse A, Maller J, Meslin C, Bonafé A, Le Bars E, de Champfleur NM, Artero S, Ancelin ML. (2012). Depression in elderly persons subject to childhood maltreatment is not modulated by corpus callosum and hippocampal loss. Journal of Affective Disorders 141(2-3):294-9.
Sun J, Maller JJ, Daskalakis ZJ, Furtado C, Fitzgerald PB. (2009). Morphology of the corpus callosum in treatment-resistant schizophrenia and major depression. Acta Psychiatrica Scandinavica 120(4):265-73.
Ternes A-M, Maller JJ, Fielding J, Addamoe P, Whited O, Georgiou-Karistiana N. (2013). Investigating the role of the corpus callosum in regulating motor overflow in multiple sclerosis. Journal of Neurology 260(8):1997-2004.